Request Call Back

The exact pathophysiology of PCOS is not clearly known. Numerous genetic & environmental factors act & contribute to its pathophysiology.
Reasons :
Excessive production of Androgen, especially from the ovaries & from the adrenals in 50 % of women.
Causes :
Excessive growth of dark & coarse hair in male-like patterns in females due to excess production or secretion of Androgen Hormone by the ovaries or Adrenal glands.
The primary culprit/wrongdoer is the Dihydrotestosterone Hormone (DHT) that comes from testosterone. The DHT hormones attack the hair follicles causing hair loss & no growth.
Occurs due to abnormal levels of Lipids in the blood.
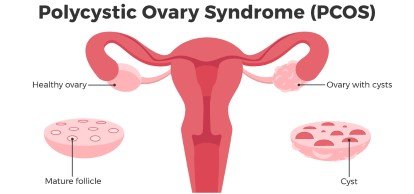
It is a condition during which females have infrequent menstrual periods. PCOS causes an imbalance in female hormonal levels along with the formation of fluid-filled cysts within the ovaries & secretion of a larger amount of male hormones called Androgen.
The absence of regular menstrual cycles is one of the symptoms of Amenorrhea. Primary Amenorrhea is when you get a delayed Menarche or you do not get your first menses within the normal age of 11 – 15 years. Secondary Amenorrhea is when a woman misses her menses for 3 months in a row or more. A woman can suffer from headache, vision changes, nausea, excessive facial hair, hair loss, changes in the breast, secretion of milky fluids of discharges from
This is a condition when a woman is not able to conceive even after having continuous unprotected coitus for a year. This may happen due to anovulation or no folliculogenesis due to PCO.
Skin thickened & pigmentation commonly appears at the nape of the neck, groins, axilla, etc. This atypical skin cell growth is most commonly triggered by high levels of insulin in the blood.
Endometrial Hyperplasia – Increased risk of Endometrial CA, Ovarian CA, Breast CA
OHSS is a complication of ART techniques. All ovulation-inducing drugs directly or indirectly increase the FSH hormonal levels. Several numbers of follicles are stimulated & each follicle releases 150 – 200 PG of Estrogen follicles. Once the follicles ovulate, they release follicular fluid containing inflammatory mediators. Vascular endothelial growth factor (VEGF) is the utmost mediator of OHSS. The most important trigger for OHSS is HCG injection.
For consultation regarding infertility treatment get an appointment at the Renew Healthcare- Best IVF clinic in kolkata




During IVF, you may hear terms like "Grade A embryo," "blastocyst quality," or "ICM and TE grading." Many couples feel...

The IVF journey can be one of the most emotionally intense experiences a couple faces. From hormone injections and medical...

Planning a pregnancy is one of the most meaningful steps in your life — but the journey doesn’t begin only...
")
Male fertility is closely associated with the health of sperm. A healthy sperm count and strong motility are essential for...

Meet Priyanka, a busy marketing professional. Lately, her periods have become heavy and unpredictable. Cramping disrupts her workday, and she’s...

Role of IVF in Overcoming Infertility Challenges in Endometriosis Endometriosis is an often painful disorder in which tissue similar to...

Journey towards parenthood Infertility and childlessness can be challenging journeys for couples to navigate. The emotional and physical toll of...

The "Save the Sibling" Program "Save the Sibling" program, a collaboration of Renew Healthcare, Cordlife, and HCG EKO offers hope...

What is PCOD? PCOD, also known as Polycystic Ovary Syndrome, is a common hormonal disorder that affects women of reproductive...

Intrauterine insemination aka IUI is a common fertility treatment that many couples opt for having a biological child. The experts...
Disclaimer :- The content shared by Renew Healthcare is intended for informational purposes only and should not be considered medical advice. For accurate diagnosis and personalized fertility care, please consult a qualified healthcare professional.